Although "fluidic actuators" had been around for a long time prior to Joseph Laws McKibben's invention, none had been used previously for prosthetic applications, yet alone robotics. It was McKibben's use that coined the term "Artificial Muscle".
Joe McKibben talks about his invention:
More Help For Polio Victims
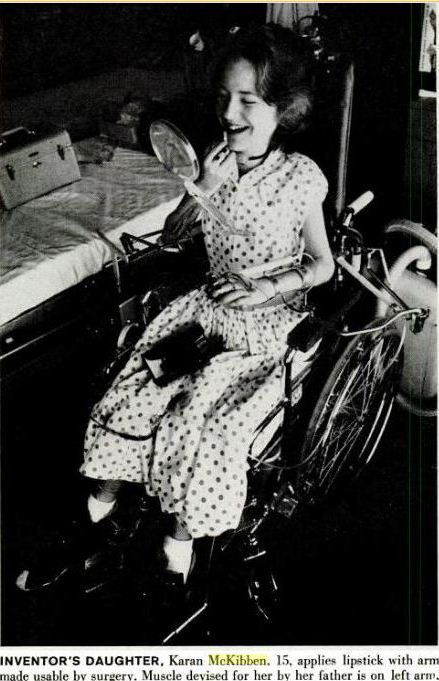
To bring motion to his little daughter's polio-paralyzed hands, Dr. Joseph Laws McKibben, an atomic physicist at Los Alamos, N.M., has developed a new mechanical "muscle" which some day may help thousands of other paralyzed fingers to move, to grasp, even to write.
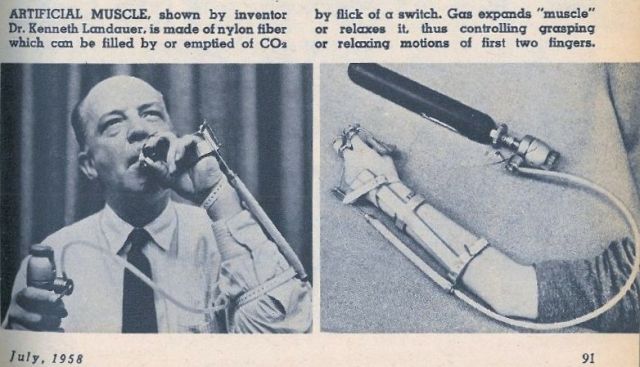
The device, a simple nylon tube, powered by bottled carbon-dioxide gas, was demonstrated for the first time at a conference on human disability. "This is the best thing we've had so far for aiding the crippled," said Dr. Kenneth Landauer of the National Foundation for Infantile Paralysis.
Dr. McKibben, 46, is the physicist who triggered the first atomic-bomb test thirteen years
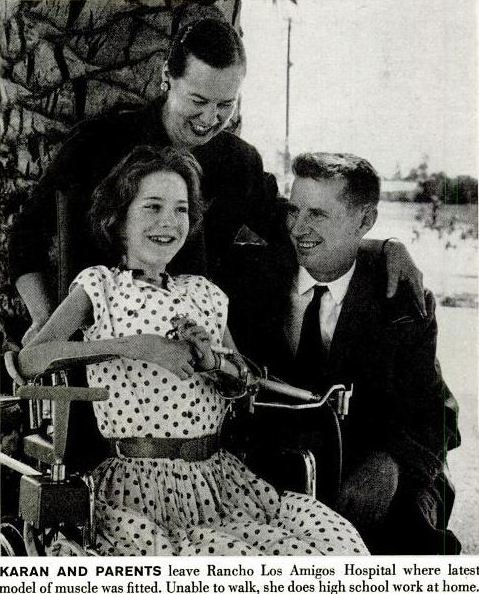
ago at Alamogordo. In 1952, his daughter Karen, now 13, 'Was stricken with polio and was paralyzed from the neck down. Since then she has lived many months in an iron lung at the Rancho Los Amigos Respiratory Center in Los Angeles, one of the fifteen rehabilitation institutions set up by the polio foundation to treat a variety of patients, including many paralyzed by polio. Last fall, Dr. Vernon Nickell, chief orthopedist at the center, asked Karen's father to make some sort of mechanical gadget that would help the girl to use her useless fingers. "I had been considering a hook for Karen's use," Dr. McKibben said last week. "But Dr. Nickell suggested some kind of mechanical 'muscle' instead."
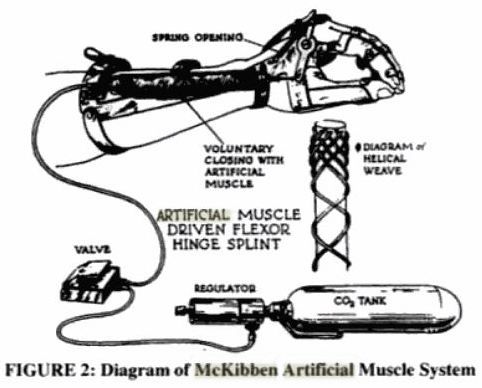
Vital Valve: After studying hydraulic, electric, and gas methods of moving paralyzed arm muscles, McKibben found a report from German scientists who had designed an ingenious pneumatic gadget operated by carbon dioxide, which inflated a bellows, thereby compressing the arm muscles and creating a pinching motion of paralyzed fingers. "It was simple enough to sketch a valve for the device," McKibben added. "After all, I'm in the business of making vacuum valves."
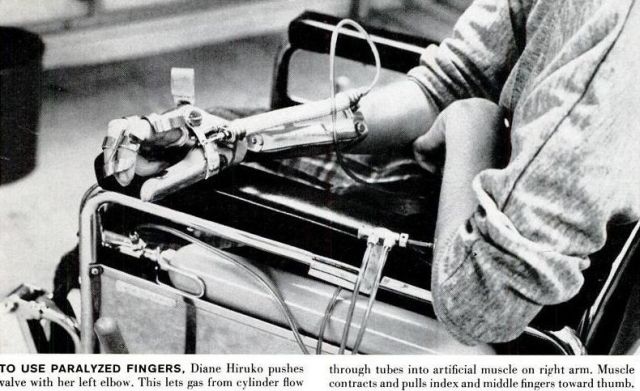
At the Rancho Los Amigos center, doctors and technicians teamed up to help McKibben perfect a workable device. As it stands now, the "muscle" is a small, rubber-lined plastic tube which lies along the paralyzed forearm and is fitted by a moving splint to the thumb and first and second fingers. When a lever is touched, gas from a 14-inch cylinder flows into the tube, causing a contracting motion, drawing the paralyzed fingers together When the lever Is touched again, the plastic tube is deflated and the fingers relax.
"The device is a wonderful source of energy. It is lightweight, simple, and safe," said Dr. Nickell.
At Rancho Los Amigos it is being used successfully on a small group of paralyzed patients. 1n New York, officials of the National Foundation for Infantile Paralysis announced that they would launch a crash research program in the hope that McKibben's invention will soon be adapted to move both paralyzed shoulders and elbows. The same theory, said Dr. Landauer, may be applicable to artificial limbs and to arms and legs that are weakened, but not paralyzed, thus offering new variety for the limited lives of cripples. When perfected, the gadget will cost less than $100. — From NEWSWEEK.
[Source: The Buckingham Post – Mar 21, 1958 – Originally from Newsweek (date unknown).]
It's interesting in that whilst the muscle itself was based on another German idea, it was the invention and utilization of the control valve that made this a workable lightweight, shoulder shrugging-controlled prosthetic arm. Even today (2012), it is the control valves that add to the complexity of usage of McKibben Muscles in robotics, orthotics, and the like. The "German idea" most likely was the development of pneumatically driven prosthetic hands and arms started in 1948 at the Orthopaedic Hospital in Heidelberg. The "Heidelberg Hand" was invented by Dr O. Häfner (Haefner).
[heidelberg pic here]
The pneumatics utilised was an expanding bellows situated within the claw-hand itself .
Another "bellows" assisted arm that may have inspired or was inspired by McKibben's Arm.
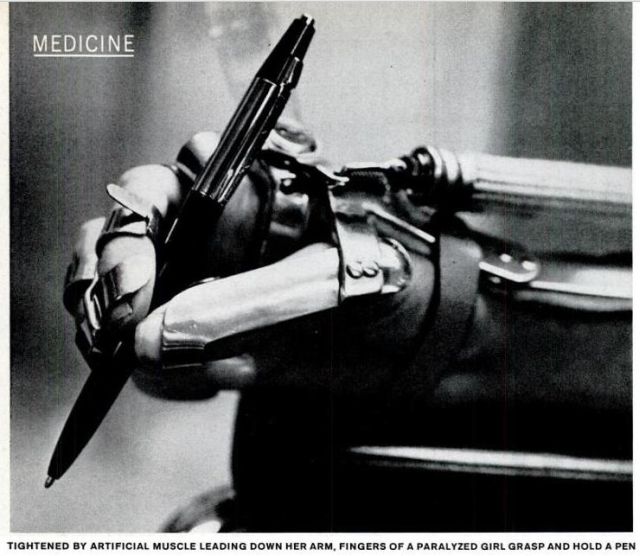
TIGHTENED BY ARTIFICIAL MUSCLE LEADING DOWN HER ARM. FINGERS OF A PARALYZED GIRL GRASP AND MOLD A PEN
ARTIFICIAL MUSCLE
No part of man's body is more distinctively human than his hand—and when it becomes paralyzed, few disabilities are more tragic. For years doctors have been looking for a substitute for hand muscles which would enable victims of paralysis to touch fingers to thumb and pick things up. The device above, developed at the Rancho Los Amigos Rehabilitation Center in Downey, Calif., solves the problem.
The artificial muscle is a sheath of woven nylon fitted over a rubber tube. Compressed gas from a cylinder is let into it by a valve which can be operated by any still usable body part. like an elbow. The gas blows up the tube, making it thicken and shorten.
When gas is released, the muscle slims and length. ens again. The muscle is harnessed to two fingers and a thumb made rigid by braces. When it shortens, they are pulled together. When it lengthens, they move apart. This is all the device does—and all it has to do to enable the user to grasp an object and let it go. The new device, permitting paralytics to eat and even type, took years to perfect. Most of the time was spent developing the braces. The muscle itself was invented four years ago by Joseph L McKibben after his daughter (below) was paralyzed by polio. McKibben is a Los Alamos physicist, famous as the man who pushed the switch to detonate the first A-bomb.
[Source: Life Magazine 14 March 1960]



[Source: La Tecnica Illustrata 1960_07 here]
Although the above article says the arm was invented by Dr Landauer, he was one of several who assisted in perfecting what's now called the "McKibben Artificial Muscle". The above example does not have the shoulder-control valve as designed and built by McKibben.
[Source: Mechanix Illustrated – July 1958]
More recent comments on the McKibben Muscle:
Spinal Cord Medicine: Principles and Practice.
Lin VW, Cardenas DD, Cutter NC, et al., editors.
New York: Demos Medical Publishing; 2003.
Historic Background
The designs for upper limb orthoses were often originally developed for patients with conditions other than SCI. One of the earliest of these was the flexor-hinge hand splint. Originally designed for the polio patient, this orthosis transmitted the force generated by active wrist extension via a mechanical linkage to paralyzed index and long fingers, enabling finger closure against the thumb (10). The design of this orthosis evolved into what today is known as the wrist-driven, wrist–hand orthosis (WDWHO)—formerly called flexor-hinge splint or tenodesis splint). This orthosis offered prehension capability that had obvious application for the SCI patient. Individuals with C6–7 lesions, with strong wrist extensors and paralyzed finger flexors, could utilize the WDWHO to improve function. The orthosis harnesses wrist extensor power and utilizes the power of wrist extension to flex the fingers at the metacarpophalangeal joints against a stable thumb.
Some patients lacked sufficient wrist extensor strength to utilize the WDWHO. The development of external powered designs led to a system that utilized a CO2-powered “artificial muscle” to provide proportionally controlled prehension. This system was designed in 1957 at Rancho Los Amigos Hospital in collaboration with Dr. Joseph McKibben, a physicist whose daughter contracted polio [RH-2012 and was paralysed since 1952]. Dubbed the “McKibben muscle,” it featured a rubber bladder, which was covered with a woven fabric. This unit was attached to the side of the WHO. When pressurized with CO2, the bladder would expand against the woven fabric and shorten in length. This in turn operated a linkage bar, which propelled the fingers into flexion against the stable thumb. A two-way valve, operated by shoulder shrugging, released the pressure to allow finger extension.
By the mid-1960s, smaller, more-powerful electric motors, brought a shift away from CO2 as a source of external power for upper limb orthoses. Electrical external power was coupled to the WDWHO through the use of cables and battery-powered motors. Again, there were obvious potential benefits to the patient with partial upper limb paralysis.
Encouraged by results of the work with the WDWHO, orthotists and biomedical engineers at Rancho Los Amigos Hospital undertook a much more ambitious project—a battery-powered, multidimensional upper extremity orthosis that would attempt to duplicate all major motions of the arm and hand. Designed using anthropometric measurements, this tongue-switch controlled device offered the opportunity for high-level tetraplegic patients to achieve greater independence in ADLs.
In practice, however, externally powered systems typically proved difficult to maintain. Without ready access to technical support personnel who could repair delicate electronic parts, the orthoses fell into disrepair and were discarded. Patient training was, therefore, crucial to the successful use of the orthoses. The complexity of orthotic design required a well-organized training program by occupational therapists. These two factors often proved a deterrent to continued use by all but the most committed patients.
Designs reverted to more simple mechanical components, which proved easier to operate and maintain. One design adapted prosthetic harnessing systems to the WDWHO. Upper limb prostheses have long been powered by the use of strapping systems that utilize contralateral shoulder protraction to operate a cable that opens the terminal device. This principle was applied to the WDWHO with limited success.
Current designs continue to utilize simple mechanical components, which are more easily maintained.
The Life and Times of Joseph Laws McKibben:
….McMillan travelled throughout the country evaluating cyclotrons that might be used for the project and chose the Harvard cyclotron as the best. Manley selected the University of Illinois' Cockcroft-Walton accelerator and two Van de Graaff accelerators at the University of Wisconsin: the "long tank," a 22-foot-long machine that could produce energies of up to 2.6 million electron-volts, and the "short tank," a 17-foot-long machine built by Joseph McKibben, a graduate physics student at the University of Wisconsin who accompanied both accelerators to Los Alamos.
JOE MCKIBBEN is an 82-year-old (as at 1995) retired Los Alamos physicist who made the final connections to the atomic bomb after it was suspended in its tower. He was the last to leave the Trinity site before the explosion.
McKibben, who still lives in the town of Los Alamos, spent the final night at ground zero to ensure the gadget wasn't tampered with. Mattresses had been laid at the tower base as a precautionary move in case the bomb fell, and at 2 a.m. McKibben lay down to get some sleep. He was awakened by a pre-dawn lightning storm that spattered him with rain.
He closed the switches at the base of the tower, drove 800 yards to a relay station and threw switches there, then came back to the tower. Because of the storm the test was pushed back an hour, to 5:30 a.m. Communication was difficult because scientists were using the same radio frequency as a nearby Voice of America station. Finally, he made his final connections and drove to his bunker about two miles away. Photo floodlights were turned on inside to allow cameras to record the final countdown.
Then the bomb went off.
"I had a photo flood on, but suddenly realized there was a lot more light coming in the back door," he recalled. "It was very brilliant outside." He threw one more switch to trigger instruments measuring the blast, then rushed outside 13 seconds after the bomb ignited. "I ran out and took a look at it. It was a big ball of fire, brilliantly colored and highly turbulent. The color was somewhere between red and purple."
What was he thinking? "I felt we had been successful in our project. I knew the war would soon be over."
Four hours after the explosion, the cruiser Indianapolis steamed out of San Francisco Bay bearing a bomb nicknamed Little Boy. It was headed for the bomber base on Tinian Island in the South Pacific, where it would be loaded on a Boeing B-29 and dropped on Hiroshima, Japan, on Aug. 6. Little Boy was not quite as powerful as Fat Man; it exploded with a force of about 16,000 tons of TNT.
After its delivery, the Indianapolis was torpedoed by a Japanese submarine and its crew was spilled into the water. More than 500 of them drowned or were devoured by sharks.
Pieces of a copy of Trinity's Fat Man, again fueled with Hanford plutonium, were delivered by air to Tinian, assembled and dropped on Nagasaki, three days after Hiroshima. It exploded with the power of 22,000 tons of TNT.
Because of the chaos and obliteration following the bombings and uncertainty about attributing cancer deaths to radiation, estimates of deaths from the two bombs range from 115,000 to 340,000. If the latter is correct — and it is closer to the historical consensus — the two "gadgets" killed more Japanese than all the Americans killed in all the battles of World War II.
They also ended a war that had, with conventional weapons, already claimed at least 40 million people. In just one horrific example, the Japanese army is estimated to have massacred as many as 200,000 Chinese civilians in Shanghai in 1937.
Would like to know if Joseph Laws McKibben is alive and well today? Met him many years ago with my family.